When I was growing up I never heard anyone claim to be born in the wrong body. But that claim is becoming increasingly common today. How can someone be born in the wrong body? Doesn’t that imply existence before birth? If so, where were they? And how could they have preferred a particular gender before they were embodied? Biological girls may also claim, “I’ve always been a boy.” What does that mean? How could they have been a boy before they were born?
Probing these claims quickly takes us into a deep and speculative realm.
Gender confusion is not just being expressed; it is being taught to young children. Check out the Gender Unicorn below used in elementary schools in the U.S.
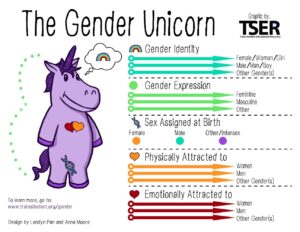
According to this cartoon, gender consists of five different elements:
- gender identity,
- gender spectrum,
- sex assigned at birth,
- physical attraction, and
- emotional attraction.
Students are even asked to come to the front of the class and indicate where they fall on the spectrum of each element.
Should young children be taught these concepts? Are these concepts even true? In terms of gamete production, don’t we have a simple binary—those who produce eggs (females) and those who produce sperm (males)?
Documentary
If you want to get a grasp of this topic, I recommend watching this excellent documentary produced by the BBC in 2017. The film shows a teenage boy who happily transitioned to being a girl as well as a girl who experienced gender dysphoria but remained a girl. In the latter case, the girl’s father shares the anguish he experienced from having to repeatedly argue with his young daughter who persistently claimed, “I’m a boy.” She would even scream and punch herself in the genitals as she made this claim. Yet, the father held his ground, and after several years, his daughter accepted her female gender.
One of the experts interviewed in the documentary is Dr. Kenneth Zucker, who has treated hundreds of children with gender dysphoria. Because Zucker did not immediately offer gender affirmation to his patients, he was accused of practicing conversion therapy and fired from Toronto’s Centre for Addiction and Mental Health (CAMH) in 2015. Many psychiatrists around the world wrote letters expressing their disapproval of CAMH’s decision. Since there was no evidence that Zucker was practicing conversion therapy, CAMH later apologized and paid him a financial settlement of more than $500,000.
Gender Dysphoria
The Diagnostic and Statistical Manual (DSM-5), the standard manual used by psychologists, presents the criteria for gender dysphoria. (Zucker served as the chair of the DSM-5 Work Group on Sexual and Gender Identity Disorders.) The DSM-5 defines gender dysphoria in children as “a marked incongruence between one’s experienced/expressed gender and assigned gender, lasting at least 6 months, as manifested by at least six of the following (one of which must be the first criterion):
- A strong desire to be of the other gender or an insistence that one is the other gender (or some alternative gender different from one’s assigned gender)
- In boys (assigned gender), a strong preference for cross-dressing or simulating female attire; or in girls (assigned gender), a strong preference for wearing only typical masculine clothing and a strong resistance to the wearing of typical feminine clothing
- A strong preference for cross-gender roles in make-believe play or fantasy play
- A strong preference for the toys, games or activities stereotypically used or engaged in by the other gender
- A strong preference for playmates of the other gender
- In boys (assigned gender), a strong rejection of typically masculine toys, games, and activities and a strong avoidance of rough-and-tumble play; or in girls (assigned gender), a strong rejection of typically feminine toys, games, and activities
- A strong dislike of one’s sexual anatomy
- A strong desire for the physical sex characteristics that match one’s experienced gender”
The condition must also be associated with “clinically significant distress or impairment in social, occupational, or other important areas of functioning.”
Gender Affirming Care
What is the treatment for gender dysphoria? Almost all U.S. accrediting organizations, including the American Medical Association, American College of Physicians, and the American Psychological Association, have adopted the affirmative care model. This model requires doctors to affirm the gender identity of the patient. It is believed that affirmative care is the only model that diminishes gender dysphoria and suicidality.
Affirmative care begins with parents assisting their child’s social transition—new name, pronouns, clothes, treatment. It progresses with medical treatment. Depending on state laws, children can take puberty blockers as early as 8 or 9 years old, cross-sex hormones at 14, and have surgery at 15 or 17.
For female-to-male transition, wearing a chest binder usually precedes a mastectomy—the removal of breast tissue. A small percentage of biological females also choose to have a phalloplasty in which a penis is constructed often by using skin from the forearm.
For male-to-female transition, surgery includes mammoplasty or breast implants, orchiectomy—removal of testicles, and vaginoplasty—construction of vagina often from penis tissue. Beyond this, lifelong medical care is required because biological nature is always trying to reassert itself so, for example, patients must continue to receive hormone therapy.
Origin of Gender Affirming Care
Why do major medical organizations think gender is changeable?
Gender identity is viewed as a social construct—the result of our culture and upbringing. Sex, on the other hand, is biological. However, even sex has components of social influence. The doctor who said you were male or female at birth could have been wrong so, it is believed, it is better to say “assigned female at birth” (AFAB) instead of “girl” and “assigned male at birth” (AMAB) instead of “boy.” Jaime Reed worked in a gender clinic in the U.S. and says she never heard the terms “girl” or “boy.”
Why is gender identity viewed as a social construct?
In her book, Material Girls, Kathleen Stock highlights eight key moments that influenced current notions, starting with a quote in Simone de Beauvoir’s 1949 book, The Second Sex, “One is not born, but rather becomes a woman.” Instead of summarizing each of the moments, I will elaborate on Moment 2.
Dr. Money and David Reimer
In 1965 the first gender identity clinic opened in the U.S. at Johns Hopkins. This clinic was staffed with New Zealand psychologist Dr. John Money and surgeon Claude Migeon who originally treated intersex children. (Intersex is a label used for about 40 variations of sexual anatomy, occurring in around 1% of the population. These include differences of chromosomes, internal reproductive organs, and external genitalia. For example, a person can be born with ovotestes, meaning they have an ovary and testicular tissue.)
But Dr. Money went beyond treating intersex children. In 1966, when David Reimer (born Bruce) was 8-months old, he had a botched circumcision that left him with a badly damaged penis. His parents took him to see Money, who recommended the following course of action for Bruce:
- remove his genitals,
- administer female hormones, and
- raise him as a girl.
Why did Money think Bruce should be raised as a girl? Because his penis was essentially destroyed and he believed gender is malleable. Boys who are raised as girls will turn out to be girls.
The Reimer’s followed Dr. Money’s advice. Bruce’s name was changed to Brenda and he was raised as a girl. Since David had an identical twin brother, Brian, this provided Money with the perfect experiment—a control group and an experimental group. Disturbingly, during regular visits to Money, the brothers were told to conduct sexual rehearsal acts with each other to help accustom them to their gender.
While “Brenda” was growing up, he was teased by peers because he wore female clothes but looked masculine. He also never felt comfortable as a girl and even urinated standing up. In his early teens, “Brenda” refused to go back to see Dr. Money, telling his dad he would commit suicide if he had to see Money again. When “Brenda” was 15 his dad finally told him the truth—he was born male. “Brenda” then changed his name to David and lived like a man and married a woman.
At the age of 36 David’s brother committed suicide; two years later David committed suicide. Meanwhile, for many years, Dr. Money had been using David’s story as support for his theory that gender is a social construct disconnected from biology. His version of the Reimer story was even used in textbooks, leading many to think that gender is a social construct. But Money’s account was the opposite of David’s reality. David could not shake his biological sex even though he was raised as a girl from infancy. Sex or gender is not as malleable as Money thought. You can listen to David and his mom tell their story here and here. And here is the go-to book on David Reimer’s life.
Criticisms of Gender Affirming Care
Criticism of gender affirmation treatment has existed for decades. In 1979 Dr. Paul McHugh ended sex reassignment surgery at Johns Hopkins Hospital. In a First Things article, he writes:
I have witnessed a great deal of damage from sex-reassignment. The children transformed from their male constitution into female roles suffered prolonged distress and misery . . . Their parents usually lived with guilt over their decisions . . . As for the adults who came to us claiming to have discovered their ‘true’ sexual identity and to have heard about sex-change operations, we psychiatrists have been distracted from studying the causes and natures of their mental misdirections by preparing them for surgery and for a life in the other sex.
It’s remarkable when a biological male or female requests the ablation of their sexual reproductive organs when they are normal,” he said. “These are perfectly normal tissue. This is not pathology.
So McHugh’s criticisms include (1) “prolonged distress and misery” and (2) doctors should not cut off “perfectly normal tissue.” Likewise, Jamie Reed worked at one of the 100 gender clinics in the U.S. She wrote an article in February 2023 titled, “I Thought I Was Saving Trans Kids. Now I’m Blowing the Whistle.” After working in the clinic for four years, she came to the conclusion that they were “permanently harming the vulnerable patients in our care” so she quit. She writes:
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
Essentially, then, after working in the field both McHugh and Reed came to the conclusion that the standard treatment harms patients.
Third, since puberty blockers, cross-sex hormones, and sex reassignment surgeries have only recently been used on a large-scale, there are no good long-term studies supporting their effectiveness and safety. Victor Sowle writes:
As of today, there exist no studies showing the long-term impacts of puberty blockers on children. Therefore, studies on the effects of puberty blockers are short-term and consist of observational data or case study reports, meaning that there is little to no evidence we can take away from them. (Gender Troubled, 71)
And,
the American Academy of Child and Adolescent Psychiatry . . . states that there have been ‘no randomized controlled trials of any treatment’ for dysphoria. There currently exists no empirically valid way of treating transgender children . . . (pg. 85)
Moreover, all surgeries have risks. For instance, an 18-year-old U.K. citizen died from complications due to a vaginoplasty.
Fourth, many who struggle with gender dysphoria have comorbidities (another mental illness). For example, more than one-third are on the autism spectrum, one-third had childhood trauma, including physical and sexual abuse, and some have depression, personality disorders, and OCD. Gender affirming, then, may not get to the root of the problem.
Fifth, Dr. Lisa Littman gathered data from 256 parent reports and expressed her findings in a 2018 paper. She discovered that 80% of the teenagers with gender dysphoria were natal females with no indicators of childhood gender dysphoria, a majority had another psychiatric diagnosis, 65% claimed to be transgender after prolonged social media use, and transgender identification within some of the girls’ friend groups exceeded 70 times the expected rate. These patterns led Dr. Littman to coin the phrase, rapid-onset gender dysphoria (ROGD) because she believes we are essentially seeing a social contagion among young girls who want to transition to male. If the cause is primarily social, the solution is not hormones and surgery. (Abigail Shrier incorporated Littman’s research into her insightful book Irreversible Damage.)
Sixth, the majority of youth (as high as 80%) with gender dysphoria desist when they become adults. Also, some who transition, subsequently regret their choice, and detransition. Keira Bell and Chloe Cole are two women who have blamed the medical system for rushing them through gender affirming care at a young age and have since returned to their birth sex. Bell even sued the world’s largest pediatric gender clinic—GIDS in the U.K.—and won. However, the case was overturned the following year. GIDS closed down in April 2023.
No one can say exactly how many transitioners regret their decision. After all the money and time invested in the transition, how many are willing to say they regret it? We do know that a Subreddit dedicated to detransition has almost 47,000 members. Sex Change Regret says “up to 20% have regrets about their ‘sex change.” It also says, “Ten to 15 years after surgical reassignment, the suicide rate is 20 times that of comparable peers.” However, others claim, “Most trans people are happy that they transitioned and 99% of trans people have no regrets about undergoing gender confirmation surgeries. A tiny minority of people do detransition and might do so for a number of reasons including family or societal rejection.” (This quote was on transactual.org, which is no longer online.)
This brings up an important point. Deciding to transition has a major impact on family and friends so this is not a decision that should be taken lightly. It is not just about the patient. Read the YouTube comments on this video to get a taste of how this issue affects relatives.
Halting Gender Affirming Care
In addition to the closing of the national gender identity clinic in the U.K. in April 2023, Finland (2021) and Sweden (2023) have begun restricting hormone treatments and surgeries for minors. In the U.S. eighteen states now have a law or policy banning affirmative care up to age 18 and twelve more states are considered passing such a law. This movement to slow down or halt gender affirmation care for young people is likely to continue.
At the same time, other states are moving in a different direction. California, Washington, and Vermont have passed laws to protect trans youth from their estranged families. Hence, they see themselves as refuge states for trans youth.
Conclusion
Adults have a right to receive whatever surgery they want to pay for, but people under 18 should not be allowed to medically transition to another gender. Here are a few reasons to support that claim:
- Most with gender dysphoria will desist when they become adults.
- Some will regret the decision and seek to detransition. But detransitioning is complicated when body parts have been removed.
- Gender dysphoria may be rooted in another mental health problem.
- There is no long-term evidence that affirmative treatment is safe or effective.
- All drugs and surgeries have side effects and risks.
- There is a strong possibility that social contagion has contributed to the rise of gender dysphoria among teenage girls in the U.S. This is fueled by social media.
Childhood and adolescence is a time of major changes so we should expect teenagers to struggle with their identity during this time. We should support them, but we should not encourage them to make life-altering decisions when their brains are not fully formed.
If this is right, almost all U.S. accrediting organization are wrong. This is a disturbing thought. How could they all be wrong? What has influenced these organizations to come to the same conclusion? We know there is a lot of money to be made in affirmative care because people need treatment for life. Is this purely a matter of greed? Scott Newgent is a trans man who believes greed is at the root of this model. See Newgent’s talk and interview.
For more information, see the fact sheets on this topic here.

After graduating from Gordon-Conwell Theological Seminary, I served as a Bible and theology teacher in Asia and the U.S. My new book explores the amazing doctrine of the Trinity.
Discover more from BibleBridge
Subscribe to get the latest posts sent to your email.